DrPlus Skin Education · Chemical Peels
Chemical Peels for Pigmentation: What Responds — and What Needs Care
Peels can fade some pigmentation beautifully and make other kinds worse. The difference is the pigment type — which is why assessment comes before acid.
How a peel fades pigmentation
Unwanted pigment is melanin that has been overproduced — after a spot, after sun exposure, after any inflammation — and deposited into the skin's cells. When that melanin sits in the epidermis, the skin's natural renewal will eventually carry it to the surface and shed it. A peel accelerates exactly this process: each session removes a controlled layer of pigmented surface cells and speeds the turnover beneath, so marks fade over weeks instead of many months.
This mechanism explains both the strengths and the limits. Peels are genuinely effective for pigment in the surface layers, and the improvement is gradual and cumulative across a course of sessions. Pigment that has dropped deeper into the dermis is beyond where a safe superficial peel works — shedding surface cells cannot reach it, which is where laser-based treatment enters the plan.
Which pigmentation responds — and which needs care
Post-inflammatory hyperpigmentation (PIH) — the flat brown marks left after acne, insect bites, rashes or minor injuries — is the peel's best patient, because the pigment is usually epidermal and the underlying cause has already passed. Surface sun damage and uneven tone respond well for the same reason. Freckles and some sun spots can lighten with peels, though laser is often the more precise tool for discrete spots.
Melasma is the pigment type that demands genuine caution. It is a reactive, hormonally influenced condition with overactive melanocytes — and inflammation is one of its triggers. An aggressive peel can therefore inflame melasma into becoming darker. That does not exclude peels entirely: gentle, superficial peels can play a supporting role inside a melasma plan built around pigment-suppressing skincare, strict photoprotection and carefully chosen laser toning. But a strong peel sold as a melasma cure is a red flag.
— Comparison
Pigment types and peel suitability
| Pigment type | Where it sits | How peels fit |
|---|---|---|
| PIH (post-acne marks) | Mostly epidermal | Responds well — a course steadily sheds pigmented cells |
| Surface sun damage / uneven tone | Epidermal | Responds well; SPF protects the result |
| Freckles & discrete sun spots | Epidermal | Can lighten; pico laser is often more precise per spot |
| Melasma | Epidermal, dermal or mixed | Caution — gentle peels only, inside a broader controlled plan |
| Deep dermal pigment | Dermal | Beyond safe peel depth — laser-based treatment territory |
PIH (post-acne marks)
- Where it sits
- Mostly epidermal
- How peels fit
- Responds well — a course steadily sheds pigmented cells
Surface sun damage / uneven tone
- Where it sits
- Epidermal
- How peels fit
- Responds well; SPF protects the result
Freckles & discrete sun spots
- Where it sits
- Epidermal
- How peels fit
- Can lighten; pico laser is often more precise per spot
Melasma
- Where it sits
- Epidermal, dermal or mixed
- How peels fit
- Caution — gentle peels only, inside a broader controlled plan
Deep dermal pigment
- Where it sits
- Dermal
- How peels fit
- Beyond safe peel depth — laser-based treatment territory
The PIH paradox: the treatment can cause the problem
Here is the loop every pigmentation patient should understand: PIH is pigment produced in response to inflammation — and a peel is a deliberate, controlled inflammation. Done correctly, the stimulus stays below the threshold that triggers melanocytes and the net effect is fading. Pushed too hard on reactive skin, the peel itself becomes the next trigger, and you trade old marks for new ones.
Asian and darker skin tones sit closer to that threshold, which is why pigment-safe protocols look deliberately unhurried: gentler acids (mandelic and lactic feature often), conservative strengths built up over a longer course, sometimes pigment-suppressing skincare beforehand, and scrupulous aftercare. Slower is not a compromise here — it is the strategy.
— Mechanism
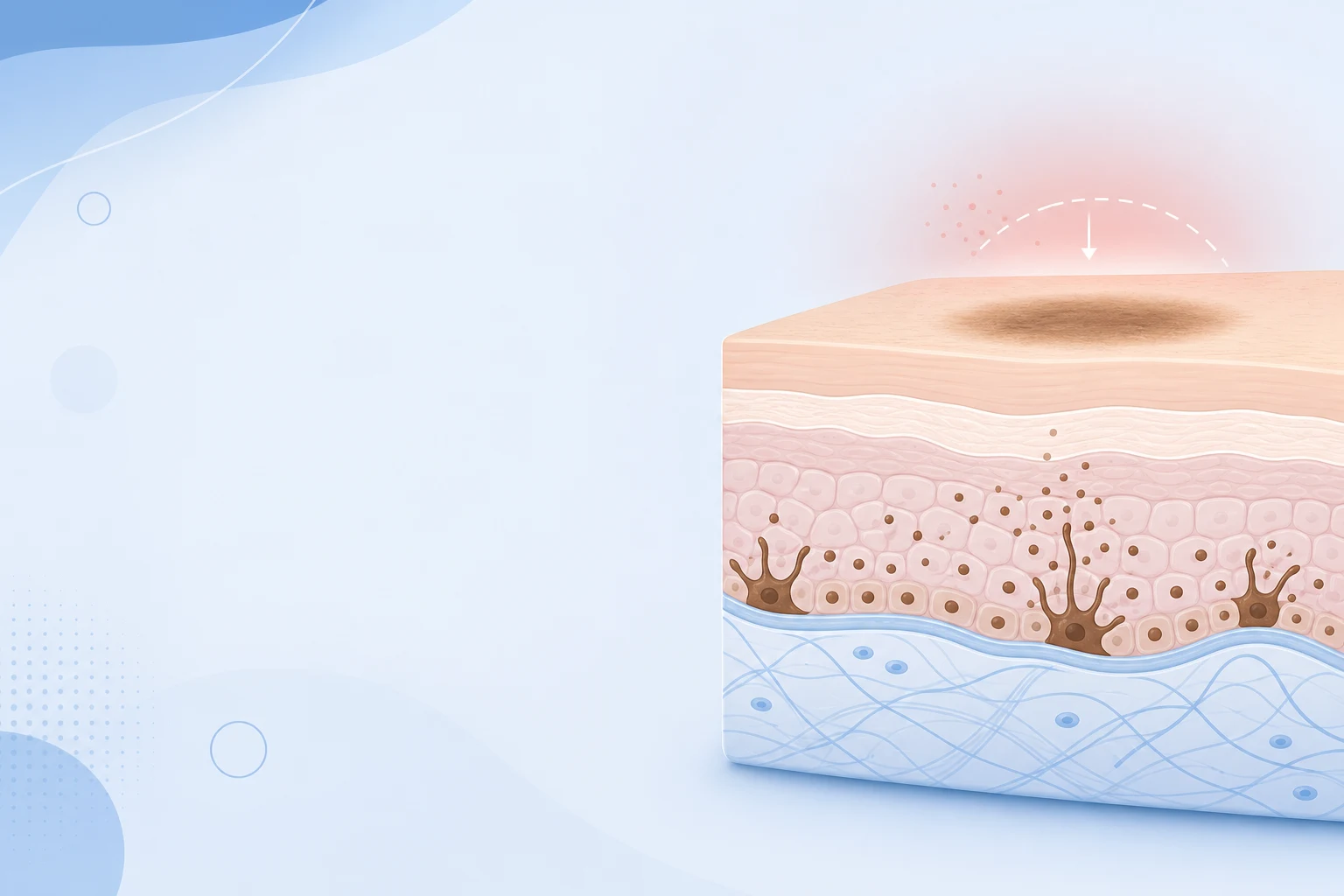
How a dark mark forms after inflammation
Inflammation
Acne, heat or a treatment irritates the skin, releasing signalling molecules.
Melanocytes activate
Those signals switch pigment cells into overdrive, over-producing melanin.
Pigment deposited
Excess melanin settles in the skin as a flat dark mark — and in deeper skin can drop into the dermis, where it fades slowly.
PIH is a pigment response, not a structural scar. It often fades over months — but the right care, and avoiding fresh inflammation, speeds recovery and prevents new marks.
Peels and pico laser: different weapons, one plan
Peels and pigment lasers attack melanin in complementary ways. A peel clears pigmented cells from the surface wholesale and speeds renewal; a picosecond laser shatters pigment particles photoacoustically so the body can clear them — including pigment sitting deeper than any safe peel reaches. Neither is universally better; they cover different depths and pigment behaviours.
In practice, many DrPlus pigmentation plans combine them: peel sessions to work the surface and keep turnover brisk, pico toning sessions for deeper or stubborn pigment, sequenced by the doctor so the skin is never doing two recoveries at once. The mix — and whether you need both at all — is decided by examining your pigment type, not by a package template.
SPF: the half of the treatment you do at home
Every pigment treatment shares a failure mode: ultraviolet light. Sun exposure is the master switch for melanin production, and freshly peeled skin is both more sun-sensitive and more pigment-reactive. Skip sunscreen during a peel course and you are refilling the pigment as fast as the peels clear it — or worse, darkening the treated areas.
The protocol is unglamorous and non-negotiable: a broad-spectrum sunscreen every morning, reapplied through the day, plus sensible shade habits — in Malaysian and Singaporean UV, all year round. Patients who treat SPF as part of the treatment keep their results; patients who treat it as optional usually meet their pigment again.
— Frequently asked
Common questions
Yes — for pigment in the surface layers. Post-inflammatory marks and surface sun damage respond well to a course of superficial peels, fading gradually and cumulatively over several sessions. Deeper dermal pigment sits beyond safe peel depth and usually needs laser-based treatment. A doctor identifies your pigment type and depth first, because that decides which tool fits.
It can, in two situations: melasma treated aggressively (inflammation is a melasma trigger), and reactive or darker skin peeled too hard, where the peel itself provokes new post-inflammatory hyperpigmentation. Both are avoidable with pigment-safe protocols — gentler acids, conservative strengths, longer courses and strict SPF — chosen by a doctor who has examined your skin.
It depends on the spot and the skin. Fading post-acne marks often suits glycolic or mandelic courses; oily, congested skin with marks may suit salicylic; darker tones often start with mandelic for its gentler penetration. Discrete sun spots may respond better to pico laser than peels. The honest answer is set at consultation, not by acid reputation.
They work differently and are often combined. Peels clear pigmented surface cells and accelerate renewal; pico laser shatters pigment particles, including deeper pigment peels cannot reach. Surface marks may only need peels; dermal or stubborn pigment leans laser; many plans sequence both. Your pigment's type and depth — assessed by a doctor — makes the call.
Most surface pigment plans run four to six sessions spaced two to four weeks apart, with visible fading building gradually across the course rather than after one visit. Deeper or mixed pigment takes longer and may need laser in combination. Progress is reviewed by the doctor, and daily SPF throughout is what protects each step of the gain.
— Related treatments
Continue with the relevant DrPlus treatment pages
Each page goes deeper into mechanism, suitability and recovery — your final plan is confirmed at consultation.
Primary money page
Chemical Peel Treatment at DrPlus
Pigment-safe peel courses selected by a doctor after examining your pigment type.
chemical peels for pigmentation concernsSupporting
Pigmentation Treatment
Assessment-led plans covering peels, laser and skincare together.
the full pigmentation treatment pathwaySupporting
Pico Laser
For dermal and stubborn pigment beyond safe peel depth.
pico laser pigment treatmentSupporting
Book a Consultation
Pigment type and depth decide the plan — assessment comes first.
have your pigment type assessed— Continue reading
 Pigmentation
PigmentationPost-Inflammatory Hyperpigmentation (PIH): Treatment Guide
Those brown marks left after a spot heals are PIH — a pigment problem, not a scar. The good news: it fades, and the right care speeds it up.
Chemical Peels for Skin Whitening: What They Really Do
"Whitening" peels do not bleach skin — they clear accumulated surface pigment so your natural baseline tone shows through. An honest guide to what that means.