DrPlus Skin Education · CO₂ Laser
Fractional CO₂ Laser for Acne Scars: Complete Scientific Guide
Fractional CO₂ laser is one of the most powerful resurfacing tools for acne scars — but only when the right scar, the right settings and the right skin meet. Here is the science behind how it actually works.
On this page
- Quick answer
- The core idea: fractional photothermolysis
- Key terms in this guide
- How CO₂ laser improves a scar
- Why the best results appear months later
- Which scars CO₂ laser suits — and which it does not
- CO₂ laser and deeper Asian skin tones
- Risks, downtime and aftercare
- How many sessions, and what to expect
- When to consider a medical consultation
- Summary
Quick answer
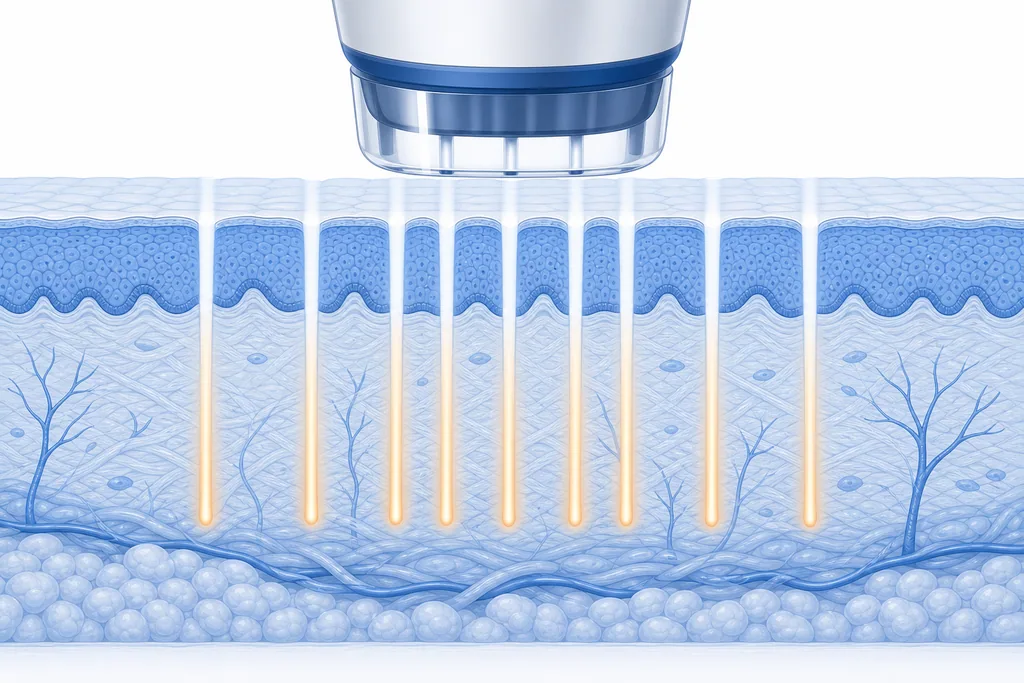
Fractional CO₂ laser is an ablative resurfacing treatment that improves acne scars in two ways at the same time. It vaporises microscopic columns of damaged tissue at the surface, and it heats the deeper dermis to trigger a wave of new collagen. The 'fractional' part means it treats only a fraction of the skin in a fine grid, leaving healthy tissue in between to heal the area quickly.
It is one of the more powerful tools for texture and for softening the walls of boxcar scars, but it is not a universal fix: deep ice pick scars and tethered rolling scars need other techniques alongside it. In deeper skin tones it must be dialled in carefully to avoid pigmentation. This guide explains the science so you can judge whether it fits your scars.
The core idea: fractional photothermolysis
The breakthrough that made laser resurfacing far safer was 'fractional photothermolysis'. Older fully-ablative lasers removed the entire surface in one pass — effective, but with long, risky recovery because the whole area had to re-heal from its edges. Fractional delivery changed the geometry: instead of treating everything, the laser fires energy in a dense grid of tiny columns called microthermal treatment zones (MTZs).
Between each treated column sits a bridge of completely untouched skin. Those bridges act as reservoirs of healthy cells that rapidly migrate in to heal the treated columns. You get a strong collagen-stimulating injury with a fraction of the downtime and risk of the old approach — which is precisely why fractional became the standard for acne scar resurfacing.
— Mechanism
Fractional vs fully ablative resurfacing
Fractional CO₂
Only narrow columns are treated. The untouched skin between them acts as a reservoir of healthy cells, so recovery is faster.
Fully ablative (older approach)
The whole surface is removed in one pass. Results can be strong, but downtime and risk are higher — a key reason fractional delivery became standard.
Simplified illustration. The depth, density and energy of treatment columns are set by your doctor based on scar depth and skin type.
Key terms in this guide
How CO₂ laser improves a scar
Two mechanisms run in parallel. First, ablation: the laser's energy is absorbed by water in the skin and instantly vaporises the targeted columns, removing damaged, irregular surface tissue. This directly refines texture and can soften the sharp upper edges of boxcar scars, where the problem is partly at the surface.
Second, and arguably more important for scars, is thermal stimulation. Around each vaporised column is a zone of heated tissue. That controlled heat is read by the skin as injury, which activates fibroblasts to lay down fresh collagen and reorganise the existing scaffold. Over the following weeks and months, this new collagen lifts and firms the depressed area from within. The visible result is the sum of surface refinement plus this slower dermal rebuild.
— Where treatments reach
Skin layers, in plain English
- Epidermis: Outer protective layer — pigmentation marks and surface texture live here.
- Dermis: Collagen and elastin layer — where atrophic scars are anchored and where most regenerative treatments work.
- Subcutis: Deeper fat / connective layer — beyond the reach of most aesthetic treatments.
A simplified illustration — actual skin layers are more nuanced. Your doctor will explain what is relevant to your case at consultation.
Why the best results appear months later
The instinct is to judge results in the first week, but that is when the skin is still red and recovering — not when the scar work is done. The collagen remodeling the laser triggered follows the body's natural wound-healing timeline, and the maturation of new, well-organised collagen continues for months after a single session.
This is why a course of treatment is usually staged: each session adds another increment of collagen and another remodeling cycle, and the sessions are spaced to let that biology run. It is also why patience genuinely matters — the temptation to treat again too soon does not speed up collagen; it only adds inflammation.
— Healing timeline
After a CO₂ laser session
Days 0–3
Ablation & inflammation
Treated skin is red, warm and may weep slightly. The body clears the vaporised columns and signals repair — this is the start of the cascade, not a setback.
Days 3–7
Re-epithelialisation
Healthy cells from the untouched bridges migrate across to close the columns. Redness peaks then begins to settle; light flaking is normal.
Weeks 2–4
Early collagen
Fibroblasts produce fresh collagen. Texture starts to look smoother as the surface heals, though deeper change is still underway.
Months 1–6
Remodeling
New collagen matures and reorganises, gradually lifting depressed scars. This slow phase is where most of the scar improvement actually happens.
A general guide only. Individual healing speed varies with skin type, scar depth, aftercare and the treatment used.
Which scars CO₂ laser suits — and which it does not
CO₂ laser is at its best on overall texture, shallow-to-moderate scarring, and the defined walls of boxcar scars, where surface ablation and dermal collagen both contribute. It is also valuable as the 'resurfacing' layer in a combination plan, refining the canvas after deeper structural work.
It has real limits, however. Deep, narrow ice pick scars often resist it because the laser cannot deliver enough energy to the base of a tight channel. Tethered rolling scars will not lift from resurfacing alone, because the laser does not release the fibrous bands pulling them down — that needs subcision first. Recognising these limits is the difference between a plan that works and one that disappoints.
— Comparison
CO₂ laser by scar type
| Scar type | CO₂ laser fit | Why |
|---|---|---|
| Boxcar | Good | Resurfacing softens the defined walls and refines texture. |
| General texture | Good | Ablation plus collagen stimulation evens the surface. |
| Rolling | Partial — combine | Helps texture but cannot release the tether; pairs with subcision. |
| Ice pick | Limited | Cannot reach the base of deep, narrow channels; needs focal techniques. |
Boxcar
- CO₂ laser fit
- Good
- Why
- Resurfacing softens the defined walls and refines texture.
General texture
- CO₂ laser fit
- Good
- Why
- Ablation plus collagen stimulation evens the surface.
Rolling
- CO₂ laser fit
- Partial — combine
- Why
- Helps texture but cannot release the tether; pairs with subcision.
Ice pick
- CO₂ laser fit
- Limited
- Why
- Cannot reach the base of deep, narrow channels; needs focal techniques.
CO₂ laser and deeper Asian skin tones
Because CO₂ laser is ablative and delivers significant heat, it carries a higher risk of post-inflammatory hyperpigmentation in melanin-rich skin (Fitzpatrick III–V), which is common across Johor Bahru and Malaysia. The pigment cells in deeper skin are easily provoked, and an over-aggressive session can trade a scar for a stubborn dark patch.
This does not rule CO₂ laser out — many people with deeper skin are treated successfully — but it changes how it is used. Expect more conservative energy and density, fewer passes, sometimes a test area, careful pre- and post-treatment skin preparation, and an absolute commitment to sun protection. For some scars and skin types, an epidermis-sparing option like RF microneedling may be preferred or used in combination.
Risks, downtime and aftercare
The most visible trade-off with CO₂ laser is downtime: redness, swelling, a sandpaper-like texture and flaking for several days to about a week, depending on intensity. Temporary risks include prolonged redness and, particularly in deeper skin, post-inflammatory hyperpigmentation. Less commonly, infection or unintended scarring can occur if aftercare is neglected or settings are too aggressive — which is why this is a doctor-led treatment, not a casual one.
Good aftercare is part of the treatment, not an afterthought. That means gentle cleansing, diligent moisturising to support the skin barrier, avoiding picking at flaking skin, and rigorous broad-spectrum sun protection — especially important under strong Malaysian sun, where unprotected skin can pigment within days. Following the plan protects the result you have invested in.
How many sessions, and what to expect
Because results depend on cumulative collagen remodeling, most acne scar plans involve a series of sessions rather than a single dramatic treatment — commonly several, spaced over months to let each remodeling cycle complete. The exact number depends on scar depth, your skin's response and whether CO₂ laser is being combined with other methods.
Set expectations on 'meaningful improvement', not 'removal'. Most people see scars become shallower and less shadowed and overall texture become smoother — often enough to make the scarring far less noticeable in everyday light. A doctor will give you a realistic range and review progress between sessions so the plan can be adjusted.
When to consider a medical consultation
CO₂ laser is powerful and ablative, so it rewards careful selection. A consultation confirms whether your scar types actually suit resurfacing, whether your skin tone calls for conservative settings or a combination approach, and what downtime to plan for.
At DrPlus in Johor Bahru, this assessment is doctor-led and honest about both potential and limits — including when CO₂ laser is best paired with subcision or RF microneedling rather than used alone, and with no pressure to proceed on the day.
Summary
Fractional CO₂ laser improves acne scars by combining surface ablation with deep thermal stimulation of collagen, all delivered in a fractional grid that keeps recovery manageable. It excels at texture and boxcar walls and is a key resurfacing layer in combination plans, but it cannot reach deep ice pick scars or release tethered rolling scars by itself.
Its strength comes with the longest downtime of the common options and a real pigmentation risk in deeper skin — both managed through conservative, staged settings and disciplined aftercare. Used well, on the right scars, it produces meaningful, cumulative improvement over months. Used as a promised one-session cure, it disappoints. A proper assessment is what tells the two apart.
— Frequently asked
Common questions
It vaporises microscopic columns of skin while leaving healthy tissue between them, and heats the surrounding dermis to trigger collagen remodeling. Surface ablation refines texture; the collagen rebuild gradually lifts depressed scars over months.
It can be, but it carries a higher risk of post-inflammatory hyperpigmentation in deeper skin. Safe use means conservative settings, fewer passes, careful skin preparation and strict sun protection — and sometimes choosing or combining with an epidermis-sparing option like RF microneedling.
Typically several days to about a week of redness, swelling, rough texture and flaking, depending on the intensity used. Your doctor will tailor settings to balance results against the downtime you can manage.
Usually several, spaced over months, because improvement depends on cumulative collagen remodeling. The exact number depends on scar depth, your skin's response and whether it is combined with other treatments.
No treatment removes acne scars completely. CO₂ laser can make scars meaningfully shallower and less noticeable and improve overall texture, but the realistic goal is softening, not erasure. Results vary between individuals.
Rolling scars are held down by fibrous bands that laser cannot release. Subcision frees those bands so the surface can rise, and CO₂ laser then refines the surface and stimulates collagen — the two address different parts of the problem.
— Related treatments
Continue with the relevant DrPlus treatment pages
Each page goes deeper into mechanism, suitability and recovery — your final plan is confirmed at consultation.
Primary money page
CO₂ Laser at DrPlus
Doctor-led CO₂ laser resurfacing — assessment, suitable settings and recovery guidance.
fractional CO₂ laser for acne scars in Johor BahruSupporting
Acne Scar Treatment Hub
The category hub where CO₂ laser is sequenced within a full scar plan.
acne scar treatment in Johor BahruSupporting
RF Microneedling
An epidermis-sparing alternative often combined with or chosen over CO₂ in deeper skin.
RF microneedling for acne scarsSupporting
Subcision
Releases tethered rolling scars before resurfacing so the surface can lift.
subcision for rolling scars— Continue reading
 Acne Scars
Acne ScarsCO₂ Laser vs RF Microneedling for Acne Scars
Two of the most common acne scar treatments — and they work in genuinely different ways. Here is how to think about them.
 Acne Scar Science
Acne Scar ScienceAcne Scar Treatment Comparison: CO₂ Laser, RF Microneedling, Subcision & Peels
There is no single 'best' acne scar treatment — only the right tool for a specific scar at a specific depth. This guide compares the four main options on the dimensions that actually decide outcomes.
 Acne Scars
Acne ScarsBoxcar Acne Scars: What They Are and Treatment Options
Boxcar scars are broad depressions with sharp, defined edges. Their shape explains why creams rarely help — and what may.